
emDOCs.net Emergency Medicine (EM) Podcast
emDOCs.net Emergency Medicine (EM) Podcast
Episode 18: Appendicitis... Why we miss it, and how do we improve?
Use Left/Right to seek, Home/End to jump to start or end. Hold shift to jump forward or backward.
Welcome to the emDOCs.net podcast with Brit Long, MD (@long_brit) and Manpreet Singh, MD (@MprizzleER)! Join us as we review our high-yield posts from our website emDOCs.net.
Today on the emDocs cast with Brit Long, MD (@long_brit) and Manpreet Singh, MD (@MprizzleER) we cover one awesome post: Appendicitis - Why we miss it, and how do we improve?
To continue to make this a worthwhile podcast for you to listen to, we appreciate any feedback and comments you may have for us. Please let us know!
Subscribe to the podcast on one of the many platforms below:
Brit: Welcome to the emDocs.net podcast. I’m Brit Long, and I’m joined by Manny Singh. Today we are covering a common condition we see in the ED, appendicitis. The original post was released on July 20th, 2020.
Abdominal pain ranks consistently among the most common reasons to visit the Emergency Department, accounting for roughly 3.4 million visits annually. Appendicitis is the most common condition requiring emergency surgical intervention, with an estimated 250,000 appendectomies performed each year. Given its prevalence, you may hear an experienced Emergency Physician (EP) proclaim that the diagnosis of appendicitis, and its disposition to the operating theater, can be reached with a thorough history and physical exam alone. But there’s more to that!
As recently as 2017, appendicitis is estimated to be missed in 4% of children and 6% of adults who present to the emergency department (3). We are missing cases of appendicitis at an unacceptably high rate in spite of its prevalence, our knowledge about it, and our ability to manage it. Why are we missing this diagnosis, and how can we improve?
Manny, let’s review the basics of appendicitis.
Manny:
Historically, the highest incidence of appendicitis occurs in 10-to-30 year-olds, with males comprising slightly more cases than females.
The appendix is attached to the posteromedial wall of the cecum. While the attachment location is consistent, the tip of this 10 cm long intestinal finger can migrate, which complicates the clinical presentation of appendicitis. It can be located retrocecal, post/pre-ilieal, subcecal, pelvis or in some cases migrate upward to present as RUQ or epigastric region.
The pathophys behind appendicitis starts as intraluminal obstruction and subsequent engorgement distal to this obstruction. This initial compression leads to activation of visceral afferent nerve fibers which produces a poorly discriminate pain in the central abdomen around the umbilicus. Eventually, bacteria multiply behind the obstruction, invade the appendix mucosa, and cause tissue necrosis, organ infarction, and eventual perforation (2). As the infection spreads into the peritoneum and bathes immediate surrounding abdominal structures, the pain “migrates” to the right lower abdominal quadrant due to somatic innervation.
How does appendicitis typically present?
Brit:
The classic symptom triad of appendicitis is: right lower quadrant abdominal pain, anorexia, and nausea/ vomiting, but it is not that straight forward. Exam findings, such as McBurney’s point tenderness, Rovsing’s sign, Obturator Sign or Psoas sign vary in their sensitivity and specificity, along with presenting symptoms such as nausea, vomiting, anorexia, abdominal pain and all symptoms.

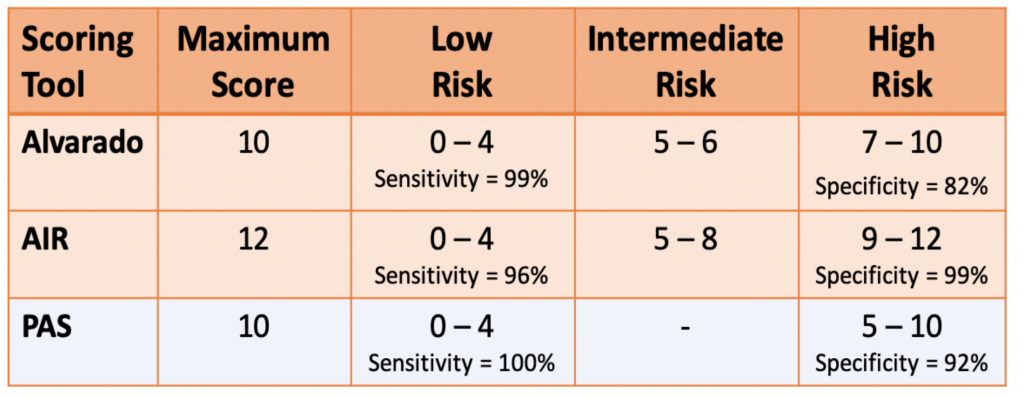
Validation tools are available to help us risk stratify appendicitis in adults and children. There’s the alvarado score, the Appendicitis Inflammatory Response (AIR) Score, and pediatric appendicitis score. Low risk patients can be discharged without further workup. Intermediate risk patients should be further observed and undergo imaging. High risk patients can reliably be taken to the OR. Sensitivity and specificity data obtained from validation studies
Although appendicitis is classically thought of as a clinical diagnosis, there is no individual sign, symptom, or lab value that can rule out appendicitis. Prior to the advent of prediction scoring systems and use of computed tomography, clinical impression alone yielded a negative appendectomy rate of 20-40% and a diagnostic accuracy of 58-92% . Judicious incorporation of labs, imaging, and prediction scoring systems has brought the negative appendectomy rate to below 2%.
So Manny, why do we miss appendicitis?
Manny:
Many emergency physicians define appendicitis within their thought process as “acute onset, migratory, right lower quadrant abdominal pain, with associated nausea, vomiting, and poor appetite, in the 10-to-30 year-old patient.” When a patient presents with this history and has tenderness at McBurney’s point, the diagnostic accuracy approaches 95%.
Therefore, the simple explanation for why we miss appendicitis is that the patient in front of us is an “outlier” to our heuristic, and we fail to consider the diagnosis as a result.
The actual factors that contribute to our diagnostic error are much more nuanced, and they are often the result of cognitive biases that we have during our workup. We also miss the diagnosis of appendicitis for unique reasons depending upon the age, gender, and even race of the patient.
Brit: Great point Manny! There are some cognitive biases that derail our decision making, as well as diagnostic errors that are unique to the “outliers” of our appendicitis heuristic.
Cognitive Biases
Cognitive bias was defined by O’Sullivan and Schofield as “cognitive shortcuts used to aid our decision making. (23)” Cognitive bias is fairly interchangeable with the term heuristic, and these “cognitive shortcuts” are frequently necessary to survive busy shifts in the emergency department. The employment of cognitive bias is not confined to the workup of appendicitis, in fact, cognitive error is estimated to be responsible for 30% of all errors within the emergency department (24). Below are several cognitive errors that we likely make when mis-diagnosing appendicitis.
Prototypical error (25):
Prototypical error is a cognitive bias that puts the clinician at risk for missing appendicitis when right lower quadrant abdominal pain is not present. For example,
Search satisfaction and confirmation bias (23):
Clinicians are also more likely to miss the diagnosis of appendicitis when they identify other pathologies first, which is known as search satisfaction. For example, clinicians




Manny, with this in mind, let’s review some of these “outliers” of our appendicitis heuristic.
Manny:
There are many populations at risk for having missed appendicitis outside the prototypical patient who is a 10 – 30-year-old male.
Children
Children ages 0–5 years have a 0.04–0.05% risk of appendectomy within the next year of life, which is 6 times lower than for children 10–20 years (4). Due to its rarity, they are 1.5 times more likely to have appendicitis missed by their doctor compared to their older pediatric counterparts (3). As a result, perforation is a more common complication in children less than 5 years who are taken to the OR for appendectomy (26).
There are limited studies investigating why young children are unreasonably at risk for this missed diagnosis. One factor may be a reluctance to utilize CT in this population given concern about ionizing radiation exposure. Given that children ages 0–5 are notoriously bad at communicating their symptoms, this reluctance is most likely due to the uneasiness that the clinician feels when dosing these young patients with a potentially mutagenic amount of radiation for a potentially inconclusive study.
This type of biased thinking is known as “omission bias” (26). Clinicians are often much more comfortable ordering an abdominal ultrasound, which is virtually risk-free. However, this imaging modality is technician-dependent and subject to a greater possibility of incomplete image of the appendix or an inconclusive result.
While the concern about radiation exposure from a CT scan is not negligible, it is worth noting that a single abdominal CT scan is equivalent to 3-years of natural background radiation. This amount can be reduced to 14-months of background radiation using techniques that reduce the scanning range to only the lower abdomen and pelvis (27,28). Given that time equals bowel, and that perforation can be rapidly fatal, physicians should consider utilizing the gold-standard imaging modality of CT scan more frequently when our suspicion for appendicitis in toddlers is high.
Brit:
Women
Women with abdominal pain are 1.68 times more likely than men to have a missed diagnosis of appendicitis (3). This discrepancy is partially due to the additional gynecological differential diagnoses that the clinician must consider when women present with RLQ pain. Particularly in women of childbearing age, mimickers of appendicitis can include ectopic pregnancy, ovarian torsion, PID, TOA, UTI, and pyelonephritis, which carry devastating possible complications of future sterility, hemorrhage, sepsis, or death if inadequately managed (17). In this situation, the list of alternative diagnoses can unsettle the clinician and bias them into working up only a subset of them, possibly at the expense of ruling out appendicitis.
Manny:
Pregnant women
Pregnant women are a subset of the female population especially at risk for missed appendicitis. Even though it is the most common non-obstetric surgical emergency, the diagnostic accuracy of appendicitis is lowest in the 2nd trimester at 64% and highest in the 3rd trimester at 88%. The high rate of misdiagnoses likely stems from the clinician’s temptation to anchor on the patient being pregnant and provide a pregnancy-related diagnosis. Anchoring bias and an incomplete grasp of normal gravid physiology create critical diagnostic errors. We can likely improve our diagnostic accuracy of appendicitis during pregnancy through awareness of this bias and by critically assessing which symptoms are appropriate during pregnancy and which are not.
For example, a common pitfall in pregnant women is to attribute nausea, vomiting, and abdominal pain to typical symptoms seen throughout normal pregnancy (29,30). In fact, nausea and vomiting are unusual after the first trimester and must be investigated as they are remain reliable indicators of appendicitis during pregnancy (30).
The pain from appendicitis is thought localize to the RUQ during pregnancy, as the appendix migrates to that quadrant secondary to uterine hypertrophy. However, researchers are beginning to question this doctrine, as studies have shown that RLQ pain remains more prevalent than RUQ in pregnant women (30,31).
Symptoms often seen in the general population, such as rebound and guarding, are less commonly encountered in pregnancy due to the abdominal wall laxity that develops to accommodate the uterus. Additionally, leukocytosis and CRP are less helpful in pregnancy since the WBC in normal gravid physiology can be as high as 16,000 cells/μL, and CRP can remain deceptively low (29).
Omission bias can appear in this population as well, due to a similar opposition to CT in pregnant women as in the pediatric population. Opponents cite the “unnecessary exposure” of the fetus to radiation, and their argument rests on a theoretical 1-in-1,000 increased chance of developing childhood cancer when abdominopelvic CT is used during pregnancy (32).
The high safety profile of ultrasound has cemented it as the first-line abdominal imaging modality during pregnancy. It is worth noting that radiology performed ultrasound carries only 63% sensitivity for appendicitis in this population and cannot be used to rule out the diagnosis (33). Thus, pregnant women with high suspicion for appendicitis and a negative US study should undergo CT (preferably reduced scan technique) as the next step in the workup, as doing so will reduce the rate of missed diagnoses.
Brit:
Elderly
In the U.S., patients older than 50 years account for 1-in-12 cases of appendicitis, yet they have a perforation rate of 28.6% as compared to 11.6% for the prototypical 10–30 year-old patient (6). The multiple alternatives bias can also explain why we miss appendicitis more often in older adults. Just as women have a unique set of diagnoses to consider, the differential for older adults must additionally include problems such as acute mesenteric ischemia, abdominal aortic aneurysm, aortic dissection, and intestinal volvulus. These diagnoses must be considered because atypical presentations of abdominal pain are more the rule than the exception due to the distinct physiology of older adults. Failure to correctly identify the cause of acute abdominal pain contributes to the 10% mortality seen in geriatric patients (34). It is essential that we perform a thorough evaluation of these patients by taking complete histories, performing broad exams, ordering thoughtful lab work, and using CT liberally.
Black Patients
Black adults with appendicitis are 1.14 times more likely to be misdiagnosed than white adults (3). The study that produced these results did not provide an explanation or hypothesis for this finding, however, racial and ethnic disparities are appreciated throughout healthcare and ED care. For example, black patients have longer ED waiting times as compared to non-black patients, black patients are assigned lower triage acuity scores than white patients, and black patients are more often treated at safety net hospitals that typically have fewer resources and higher patient volume (35,36,37). There are likely many cognitive biases and institution-wide disparities affecting the discrepancy between black and non-black rates of missed appendicitis. As EPs, we can close the gap in diagnostic error by acknowledging that we are missing a disproportionate number of cases in this population.
Why does it matter? How do we improve?
Manny:
For every 100 return visits to the ED for abdominal pain, one-third of them will be due to diagnostic error, and 2 will be for missed appendicitis (38). Once appendicitis begins, given time, it invariably leads to perforation which can be complicated by peritonitis or sepsis. Missing the diagnosis of appendicitis during a patient’s initial presentation puts them at risk for these dangerous complications, for which they will likely present to the ED again several hours to days after discharge. These repeat visits are associated with longer hospital stays with higher rates of morbidity and mortality (26). Delayed diagnosis and its complications account for why missed appendicitis is among the top three conditions cited in malpractice insurance claims in adults and children (39).
Appendicitis is a straightforward diagnosis and well within our scope of practice as long as we keep our index of suspicion high. In fact, EPs and surgeons have equal capability to diagnose appendicitis, and studies show a negligible difference in rates of complications for patients diagnosed by EPs versus surgeons (40). Lowering the rate of missed appendicitis in the ED can be accomplished through improving our awareness of cognitive biases that affect our medical decision making, being mindful of the populations especially at risk for this missed diagnosis, and utilizing all labs and imaging at our disposal when suspicion for appendicitis is high.
Brit:
Pearls
#1: Utilize prediction scoring tools: AIR score for high risk patients, Alvarado score for dischargeable patients.
These tools can reduce cognitive bias by enabling us to work up the disease objectively using the same criteria for every patient, and they are especially useful for prompting further workup for patients classified as intermediate risk. The AIR score has been shown to outperform Alvarado in identifying high risk patients (41).
#2: Don’t be afraid to utilize CT imaging for intermediate risk patients, including pregnant women and children.
The overwhelming majority of missed appendicitis is in “intermediate risk” patients. In intermediate risk patients who you still have a high suspicion for appendicitis after negative or inconclusive ultrasound, get the CT. You will “rule-in” appendicitis 9 times out of 10.
#3: Train yourself to consider appendicitis in “outlier” populations: children, pregnant women, older adults, and black patients.
If we wish to decrease the misdiagnosis rate of appendicitis among “all comers” to the emergency department, then we must remain vigilant for the diagnosis in these populations.
Manny: That rounds out our summary of this great post on appendicitis. Thanks for joining us on the podcast, and stay tuned for our next episode. Feel free to comment on our site and let us know if you have any feedback. Stay safe and healthy everyone!